Often contrary to their teenage counterparts, adult patients typically seek treatment that is greatly focused on aesthetics and consequently tend to shy away from fixed appliances. Due to their greatly improved aesthetics, clear aligners and transparent brackets have risen in popularity. Recent advances in aligner treatment have addressed the traditional critiques of slower procedures and less anchorage, leading to greater efficiency and comfort during the treatment process.
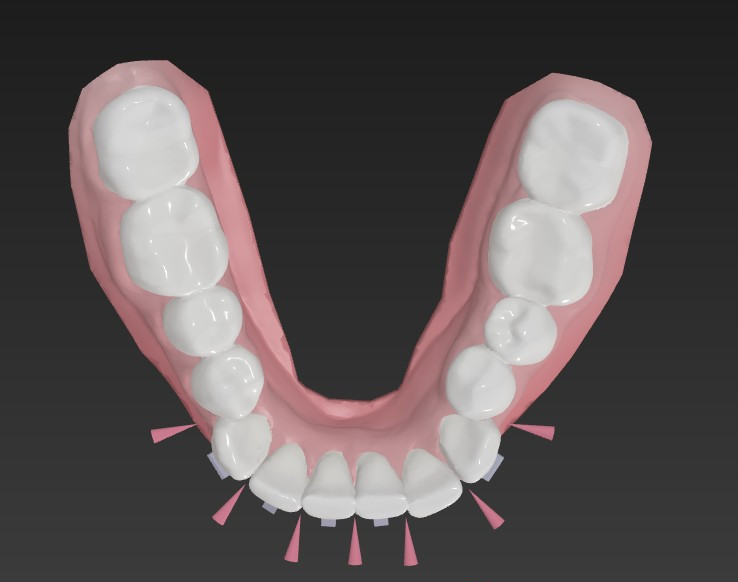
Further, intra-oral scanning has been widely adopted in orthodontic treatment, not only to aid in the ease of impression procedures, but also to serve as a visual communication tool. Communication with adult patients, especially in setting expectations regarding treatment, has been greatly facilitated by the digital workflow, including intra-oral scanning and visual representation of anticipated outcomes.
Treating adult patients often has unique challenges, including heavily restored dentition, periodontal concerns, medical complexity, long-term parafunctional habits and lifestyle choices such as smoking or consuming alcohol. Many clinicians have turned to aligners as a solution for adult treatment, owing to comfort, ease of hygiene, lack of dietary restrictions on hard and crunchy foods, and communication of expected treatment results. The purpose of this article is to discuss the use of aligner treatment in adult patients and factors that support the use of aligners.
Patient history and clinical findings
A 66-year-old female patient presented for orthodontic consultation as a referral from the prosthodontist treating her. The patient reported past bilateral temporomandibular joint pain associated with bruxism. She had undergone successful splint therapy for temporomandibular disorder (TMD) symptoms and was comfortable with her occlusion, and had a history of lichen planus that was monitored and well controlled. She felt that the crossbite of the mandibular right canine was causing interference with her jaw movement and that her teeth were shifting and the crossbite was becoming worse. The patient expressed a strong interest in aligner treatment so that she would be able to enjoy foods that are to be avoided with fixed appliances and to perform proper oral hygiene. There were also concerns for the potential of mucosal irritation with fixed appliances, and her history of lichen planus.
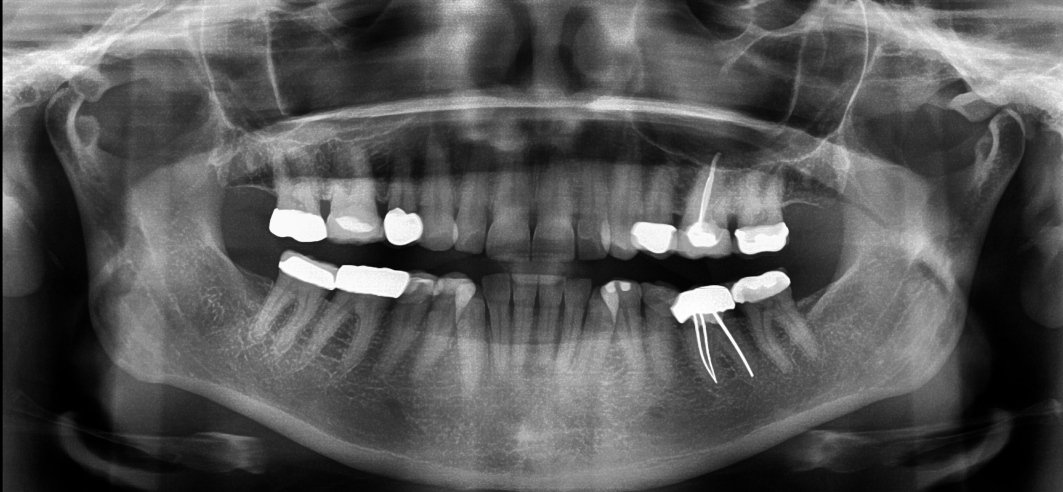
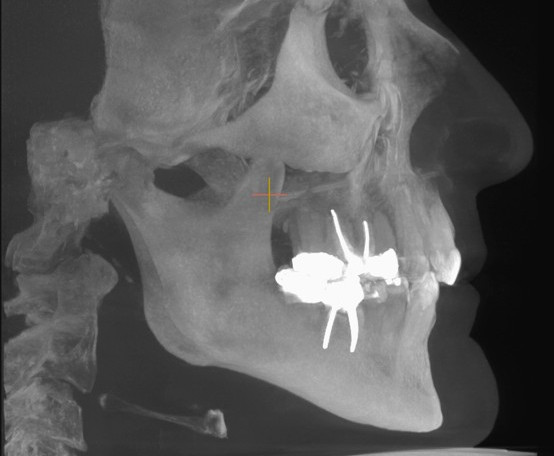
The patient reported orthodontic treatment as a teenager and extraction of two maxillary teeth. Upon examination, both gold and porcelain crowns, several composite restorations and previous extraction of the maxillary first premolars were observed (Figs. 1a–e). She presented with an Angle Class II molar relationship and Class I canine relationship. The mandibular right canine was confirmed to be in crossbite. There was a moderate overbite of 50%, and the mandibular incisors were tipped lingually, creating 4 mm of overjet. The patient appeared to have a relapse of Class II, Division 2 malocclusion in the maxillary arch, evidenced by loss of torque of the central incisors and flaring of the lateral incisors. She had mild crowding in the maxillary arch and moderate crowding in the mandibular arch. The arches lacked symmetry, the maxillary arch being round and the mandibular arch square. The maxillary midline was centred to the face, and the mandibular midline was shifted right by 3 mm. There was no detectable shift between centric occlusion and centric relation, and the patient had been restored to a cusp-to-fossa functional relationship. The patient appeared to have a restricted envelope of function due to the crossbite of the mandibular right canine and the Class II, Division 2 relapse of the maxillary malocclusion.

 International / International
International / International
 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 India / भारत गणराज्य
India / भारत गणराज्य
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
 Middle East / Middle East
Middle East / Middle East

 Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar
Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar


 Prof. Dr. Wael Att, Dr. Kubra Kundak, Dr. Acela MartinezLive webinar
Prof. Dr. Wael Att, Dr. Kubra Kundak, Dr. Acela MartinezLive webinar
 Cat EdneyRegister now1CELive webinar
Cat EdneyRegister now1CELive webinar
 Dr. Allen Wong DDS, EdD, DABSCDRegister now1CE
Dr. Allen Wong DDS, EdD, DABSCDRegister now1CE






















.")













.")





























To post a reply please login or register